On Monday, June 19, the BBC's flagship current affairs programme,
Panorama, broadcast the long-awaited, and much anticipated 'The
Antidepressant Story'.
Living, as I do, in Central America, it's difficult to watch British TV, especially live broadcasts. With the help of a useful app, however, I didn't fret too much.
While most of Britain settled down at 8pm on Juneteenth, the time difference here meant a 2pm viewing here for me.
I watched with my partner, who also has an interest, given her daughter died at
the hands of antidepressants.
Many, reading this, will know I've been banging the drum for over 16 years regarding the safety and efficacy of SSRIs so watching this hour-long special saw me (internally) go through a range of emotions. It's only now, some three days after it aired, that I'm able to write about it.
My main focus has always been about the withdrawal effects of SSRIs and also
their propensity to induce suicidality. Although 'The Antidepressant
Story' covered the withdrawal issue they never delved into the suicide
link. I totally understand why as this has been covered four times
(brilliantly) by the Panorama team during the first ten or so years of the
2000's (Links at the foot of this post)
I watched with interest as they covered PSSD. For me PSSD is a confusing
acronym, at first glance it looks like PTSD, an invented disorder that promotes
the use of psychiatric drugs. If an experienced old fella like me, who's
researched these SSRIs for many years, finds this confusing, I have to wonder
if the same can be said about the general public?
The two acronyms are very different though.
PSSD is Post-SSRI sexual dysfunction, a condition caused by the use of one or more serotonergic antidepressants that persists despite the cessation of antidepressant treatment. PTSD is Post-traumatic stress disorder, an apparent "mental health" condition that's triggered by a terrifying event.
Although I agree many suffer when recalling terrifying events, I refuse to give
it a mental health label. PTSD first appeared in 1980 in the third edition
of the Diagnostic and Statistical Manual of Mental Disorders (DSM-lll)
published by the American Psychiatric Association, a manual used by
psychiatrists, such as the ones who appeared (for balance) in 'The
Antidepressant Story', namely Wendy Burn and Prof David Nutt. More about them
later.
The Antidepressant Story kicks off with Audrey Bahrick, a patient who tells her story about reading about Prozac and its beneficial properties. She was going through a sticky patch at the time and thought Prozac would give her the lift that she needed. After taking it, Bahrick felt "confident and energized", adding, "I loved being on Prozac."
Another patient, Trish Matthews, also tells her story. Trish was training as a nurse in the 1990's and found the pressure of training whilst trying to manage her homelife, she became stressed and struggled to manage her daily life. She went to her doctor and was prescribed an antidepressant. She believed, after reading various articles, that her stress was brought on by a chemical imbalance.
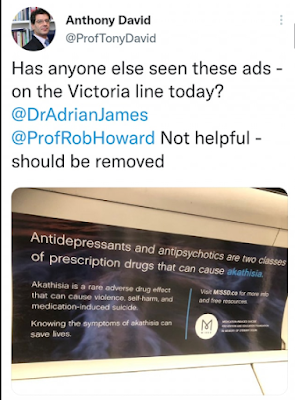
Drug company adverts, such as the one below, were flooding TV stations across
the US and New Zealand (The only two countries that allow Pharma Drug To
Consumer advertising)
It wasn't long before those adverts turned to print so other nations,
such as the UK, could read about an apparent serotonin deficiency and how to
treat it.
It was genius marketing by the drug industry but it was pure fiction, a fiction
that was lapped up by the likes of the Royal College of Psychiatrists and its
members. They never once questioned it. They could now prescribe en masse and
give a reason, albeit fictional, why they were prescribing.
The chemical imbalance myth has been debunked so many times over the years. That I'm still writing about it baffles me. It's ingrained in society, moreover in rooms with pens and prescription pads. It's cult-like and many who are hanging on to this claim are part of that cult.
Back to Bahrick and Matthews
As the show progresses we learn that Audrey Bahrick and Trish Matthews both started to experience the dark side of the SSRIs they were prescribed.
"I was immediately sexually numb, within a day (of taking Prozac) my
genitals were numb", Bahrick said.
Trish Matthews had been taking her prescribed SSRIs for 18 months and felt she
was now better so decided to cease taking them. This is when her problems
began. "Within 24 hours I felt absolutely dreadful", she thought her
'depression' was coming back. She rang her doctor who told her, "you
have to go back on them."
Withdrawing from SSRIs can mimic the symptoms of why you were put on them in the first place. Prescribers are, largely, unaware of this as are those who take them.
Dr Mark Horowitz, a trainee psychiatrist, who also features in the show, was diagnosed with depression at the age of 21. 15 years later he tried to come off and experienced insomnia, panic attacks, dizziness, anxiety and low mood. He has not been taught about these effects of SSRIs at medical school or in psychiatry training. Horowitz, when reading the academic literature available to him, found that psychiatrists and academics at the institution he had studied at and others like them around the world had little helpful to say about withdrawal effects from antidepressants, they recommended stopping the drugs over 2 to 4 weeks, and reported that the symptoms were mild and brief. To date, Horowitz is still taking his medication.
Joanna Moncrieff, a practising professor of psychiatry and a part-time academic and author, says she was skeptical about these new antidepressants from the start. "My interest has always been in the role of drug treatment and whether they're as beneficial as we are, usually, led to believe that they are."
Pfizer, who are never out of the news these days, are briefly featured in the show. The Panorama team obtained a 'secret document' that showed how Pfizer execs wanted to play down the withdrawal issue. They also wanted to include claims about the chemical imbalance being a fact, they were declined by drug regulators but the chemical imbalance somehow made its way into the patient information leaflets that accompany SSRIs. With trickery, using wordplay, companies like Pfizer could set the 'chemical imbalance' promotion rolling by putting its main message amongst words like 'it is thought' or 'it may be'. Moncrieff was shown the document by the Panorama team, her reaction said it all, "Oh, my gosh".

Moncrieff has been instrumental in trying to debunk the chemical imbalance theory and in 2022, along with Benjamin Ang and Mark Horowitz, published a paper in the Science Direct Journal that found the field of psychiatry bears some responsibility for dissemination of the theory of the chemical imbalance and associated antidepressant use.
This paper caused outrage amongst many leading psychiatrists and they took to Twitter not only to refute the findings but to target Moncrieff personally. I've watched it all unfold via my own Twitter account - it still continues today.
The Balance
As I mentioned previously, for balance Panorama asked two psychiatrists onto the show. The pharma conflicted Prof David Nutt and the former President of the Royal College of Psychiatrists, Wendy Burn.
As was expected both made claims that could not be backed up with evidence.
Nutt opted to go down the emotive route with, "antidepressants have saved
the lives of many hundreds of thousands of people”.
I find this claim astonishing and am bamboozled that it's rarely challenged by
mainstream media or, indeed, programme makers such as Panorama.
As I wrote on Twitter, "If I believed listening to the Dixie Chicks whilst going through severe Paxil withdrawal saved my life, would this actually prove that the Dixie Chicks saved my life?"
Of course it wouldn't.
There is no scientific evidence that antidepressants save lives. Too many people are scared to challenge the narrative because many patients who believe this to be true will get emotional and throw hissy fits on social media platforms. Trust me, I have friends who think they or their kids' lives were saved by SSRIs. I cannot debate with them as it causes them obvious distress.
Nutt knows this. He seems to be playing the system here, it's clever deception. Appear to have concern and show support whilst dismissing the likes of the patients that appeared in the show and millions of others who have suffered the darker side of SSRIs.
Burn didn't fare much better. Fidgeting throughout her (edited) interview, Burn said she personally regrets that severe and long-lasting withdrawal wasn't recognised sooner. "I can't really explain why it took so long, perhaps partly because of the overlap between relapse and withdrawal...I don't know, I can't really explain it."
What Panorama didn't show the public, because they probably didn't know, is an interview Burn did with Equally Well back in 2020. She told them that "when she was first trained she was told not to tell patients about side effects as it might dissuade them from taking medication."

The BBC didn't push Burn on why she has blocked or muted so many patients on Twitter who have reached out for help regarding withdrawal and PSSD issues.
Burn offered a personal apology on the show but it reminded me of Alan
Partridge publicly apologising to Norfolk farmers. "If there's anybody
watching who has gone through withdrawal and it wasn't recognized then I'm very
sorry."
You'll notice she was making a personal apology here and not one on behalf of
The Royal College of Psychiatrists, whose members with Twitter accounts are
some of the most vile human beings I've come across regarding those injured by
SSRIs. That's another blog though.
All in all, I thought the one-hour special did the job, it got the message
across and, as predicted, infuriated many Royal College members on Twitter.
Their anger was aimed at the apparent bias of the show. At no point did they
show any empathy whatsoever to those harmed by the very same drugs they
write prescriptions for. Targeting their cultish beliefs was deemed, it
seems, unacceptable.
Psychiatry is in a mess but I can't let General Practitioners (GPs) off the
hook here either. For too long now, GPs have ignored the SSRI withdrawal and
PSSD issues as have the British Drug Regulator the MHRA. This needs to change, and it needs to change right now!
I sat down with the MHRA 15 years ago to discuss the SSRI withdrawal issue,
back then I had no Facebook or Twitter support groups to help me, nor did I
have any interest from the BBC or any other network channel. I made the visit
alone and sat with the, then, chief executive of the MHRA, Kent Woods,
their Head of Pharmacovigilance Risk Management, Sarah Morgan, and
their Communication Manager, John Watkins.
I thought I'd struck gold, sadly that wasn't the case. The problem still exists
today and many patients who are prescribed these drugs will, no doubt, go
through what I did, what the patients in the show did, and what many millions
of people worldwide are having to endure.
With that said, if you want to become an advocate for SSRI safety, it comes at
a price. Members of the Royal College of Psychiatry have labelled me 'a
conspiracy theorist', a 'far-right sympathizer', a
'misogynist', amongst many other labels designed to keep me quiet. It's
straight from the pharma playbook, folks!
I'm not alone, many other SSRI safety advocates have had their fair share of crap thrown at them as they strive for answers, many of whom who have lost loved ones due to SSRI induced suicides.
The Royal College of Psychiatrists were 'royally' kicked in the nuts with this Panorama offering. It's going to get a lot worse with the insults, the accusations, the muting and the blocking. Cults don't like their belief system tarnished.
Watch the 'The Antidepressant Story' on BBC IPlayer here.
Outside the UK, watch here
Previous Panorama SSRI coverage
The Secrets Of The Drug Trials